
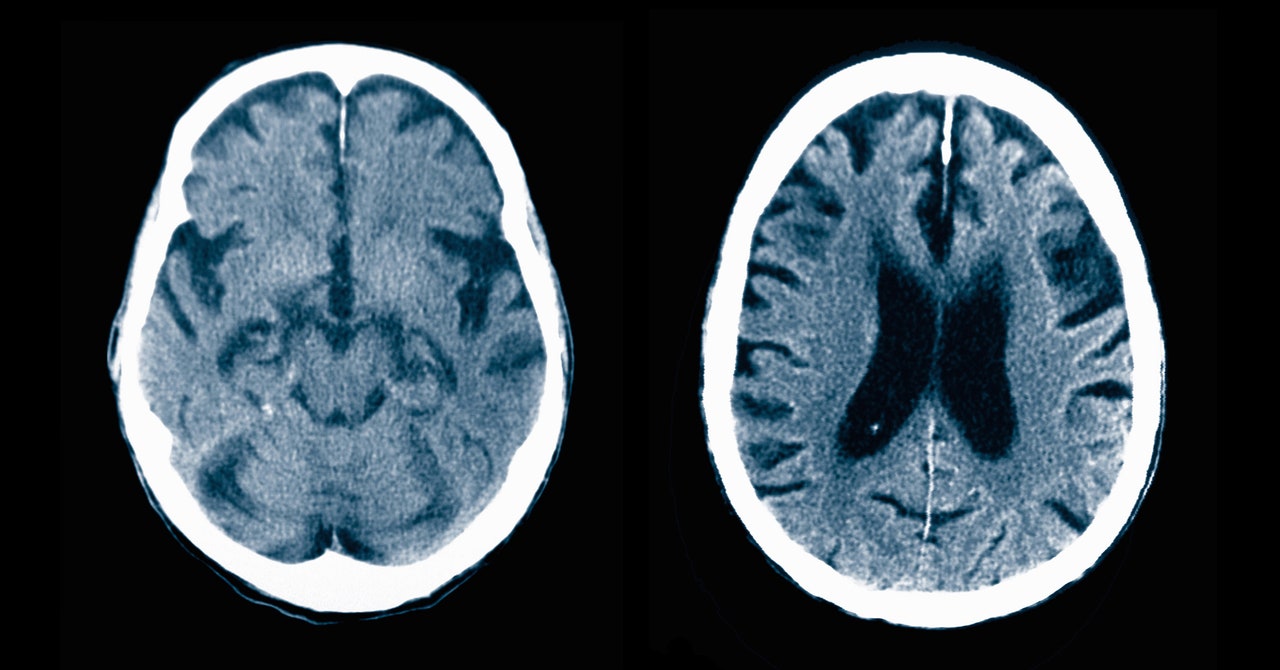
Millions of older adults likely have minor memory issues that can later become dementia. But only a fraction of them are diagnosed early enough for new treatments to stand a chance.
Millions of people over the age of 65 likely have mild cognitive impairment, or MCI—minor problems with memory or decisionmaking that can, over time, turn into dementia. But a pair of recent studies both concluded that 92 percent of people experiencing MCI in the United States are not getting diagnosed at an early stage, preventing them from accessing new Alzheimer’s treatments that may be able to slow cognitive decline if it’s caught soon enough.
“We knew it was bad. But we didn’t know it was that bad,” says Ying Liu, a statistician at the University of Southern California Dornsife’s Center for Economic and Social Research and a researcher on both studies.
Nearly anyone with mild anything goes undiagnosed.
I recognized this in my mom. She has yet to mention anything to her doctor. She refuses to believe it’s an issue.
From her point of view 1. It’s really scary. 2. Even if diagnosed, there’s not much that can typically be done.
I can understand why she would prefer to not acknowledge it
I see this in my office constantly and there are lots of reasons surrounding it. All of my patients get a mini mental status exam (MMSE) with their yearly physical after age 65.The ones with any impairment tend to deny it as real. If there is impairment, I try to work it up with labs and then a brain MRI. Insurance won’t cover a brain MRI for MCI, so it has to be coded as “memory loss”. Memantine and donepizil are not indicated for MCI, just dementia, so we don’t prescribe them that early. We wait until it progresses. Also, I’ve seen a ton of patients over the years who have “microvasular changes” on brain imaging done for other reasons that no one has discussed with them, much less actually done an appropriate cognitive assessment and further workup. I don’t know why I am such an outlier in these areas, because I’m not doing things that aren’t indicated by specialty recommendation. I think it’s just another sign of our broken system.
Any suggestions for someone with a parent who openly acknowledges that he’s having cognitive changes / difficulties? I get the sense he’s experiencing precisely this kind of pre-dementia decline. He’s on Medicare, FWIW. I just assumed nothing was realistically available (thanks, US healthcare system for the deep sense of futility), but would love to be wrong.
Okay, so how can someone in their 30s get this exam?
And here i thought they just go into politics.
Looks like some drug companies are looking to grow their market.
Those “new drugs” arent all that successful.
Memantine, donepezil, etc. should be started much earlier in this population. We need better MCI tests. My grandmother who watched both of her parents die of Alzheimer’s was passing her clinical MCI long after we had taken her keys because she was repeating questions over and over, and her house was covered in post-it notes to remind her about her post-it notes.
Our current clinical assessments for MCI are really bad.
Those are symptomatic medications. They don’t alter the course Alzheimer’s in any way. You won’t die any sooner or later from Alzheimer’s whether you’re on or off those. I’m not saying don’t offer them to people who are symptomatic and want them. I just point this out so people don’t stress too much about these. Many people don’t find them helpful and that’s fine. If they do find them helpful, that’s fine too. They have side effects, don’t alter the disease course, so they may not be right for everyone.
You could argue maybe some of the newer anti amyloid medications theoretically slow progression some, but the evidence on those is very weak at the moment. I’m still surprised either of them were approved. The first one that was approved led to most members of the fda scientific advisory panel resigning (they had recommend against). I personally would have liked to see much better hard evidence before we embark on an epic project of doing amyloid pet scans, frequent monitoring mris, regular infusions, all while adding risks of brain inflammation and brain hemorrhages, for millions of people every year, all at the cost of hundreds of billions of year (if this actually started to be done across the board). I think in our desperation to address some of these devastating diseases we may inadvertently expose people to too many risks and costs for too little benefit.
Who said anything about replacing clinical MCI exams with invasive scans? (I’m terrible; I didn’t read the article. I wouldn’t agree with replacing exams with invasive scans.) We just need better MCI exams. The ones we have now are flawed. They are not catching people who are clearly already symptomatic, and who therefore should be started on one of the existing options for small molecule drugs.
Also all of our current research uses the existing MCI exams for assessment and often endpoint, which deeply complicates things if the exams don’t even catch what they were intended to catch.
These are the requirements to use the new anti amyloid drugs (the ones that purportedly do change disease progression, unlike current small molecule drugs), which need amyloid pet imaging plus regular mris to monitor for complications. Sorry if I was unclear.


