
0
The serotonin theory of depression: a systematic umbrella review of the evidence - Molecular Psychiatry
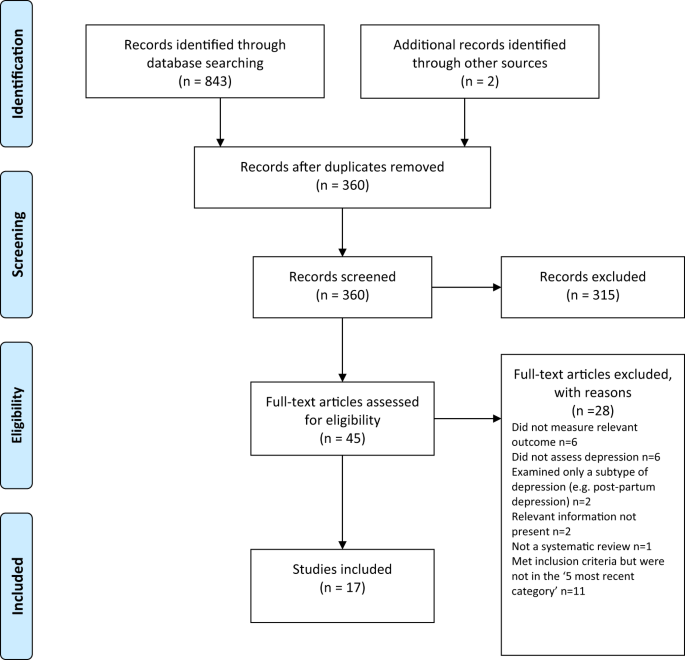
www.nature.comThe serotonin hypothesis of depression is still influential. We aimed to synthesise and evaluate evidence on whether depression is associated with lowered serotonin concentration or activity in a systematic umbrella review of the principal relevant areas of research. PubMed, EMBASE and PsycINFO were searched using terms appropriate to each area of research, from their inception until December 2020. Systematic reviews, meta-analyses and large data-set analyses in the following areas were identified: serotonin and serotonin metabolite, 5-HIAA, concentrations in body fluids; serotonin 5-HT1A receptor binding; serotonin transporter (SERT) levels measured by imaging or at post-mortem; tryptophan depletion studies; SERT gene associations and SERT gene-environment interactions. Studies of depression associated with physical conditions and specific subtypes of depression (e.g. bipolar depression) were excluded. Two independent reviewers extracted the data and assessed the quality of included studies using the AMSTAR-2, an adapted AMSTAR-2, or the STREGA for a large genetic study. The certainty of study results was assessed using a modified version of the GRADE. We did not synthesise results of individual meta-analyses because they included overlapping studies. The review was registered with PROSPERO (CRD42020207203). 17 studies were included: 12 systematic reviews and meta-analyses, 1 collaborative meta-analysis, 1 meta-analysis of large cohort studies, 1 systematic review and narrative synthesis, 1 genetic association study and 1 umbrella review. Quality of reviews was variable with some genetic studies of high quality. Two meta-analyses of overlapping studies examining the serotonin metabolite, 5-HIAA, showed no association with depression (largest n = 1002). One meta-analysis of cohort studies of plasma serotonin showed no relationship with depression, and evidence that lowered serotonin concentration was associated with antidepressant use (n = 1869). Two meta-analyses of overlapping studies examining the 5-HT1A receptor (largest n = 561), and three meta-analyses of overlapping studies examining SERT binding (largest n = 1845) showed weak and inconsistent evidence of reduced binding in some areas, which would be consistent with increased synaptic availability of serotonin in people with depression, if this was the original, causal abnormaly. However, effects of prior antidepressant use were not reliably excluded. One meta-analysis of tryptophan depletion studies found no effect in most healthy volunteers (n = 566), but weak evidence of an effect in those with a family history of depression (n = 75). Another systematic review (n = 342) and a sample of ten subsequent studies (n = 407) found no effect in volunteers. No systematic review of tryptophan depletion studies has been performed since 2007. The two largest and highest quality studies of the SERT gene, one genetic association study (n = 115,257) and one collaborative meta-analysis (n = 43,165), revealed no evidence of an association with depression, or of an interaction between genotype, stress and depression. The main areas of serotonin research provide no consistent evidence of there being an association between serotonin and depression, and no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations. Some evidence was consistent with the possibility that long-term antidepressant use reduces serotonin concentration.
This has been known for more than a decade (this study is just a review of existing research), and is not directly related to the efficacy of SSRIs (although the serotonin “theory” might have led to their adoption, idk).
For a while now, as I understand it, the view has been that SSRIs cause the downregulation (decreased new production of) serotonin receptors in reaction to the excess serotonin buildup they cause in the synapses (this is why they take a few weeks to kick in, despite increasing serotonin levels almost immediately, and is also why they will desensitive you to psychedelics like LSD, which act primarily on serotonin receptors). They decrease overall serotonin signalling, which in turn has downstream effects that alter certain activites of certain regions of the brain that are implicated in depression. (This is based mostly on discussions I had with my psychiatrist a few months ago, so if there are any actual experts here, correct me if I’m wrong.)
That being said, SSRIs suck ass, their side effects are awful, and I think it’s medical malpractice to make them a first-line treatment tbh. It’s really mind-boggling that they’re the go-to given how much shit they fuck up.
I love reading about their effects on libido including doctors “joking” to women about how they won’t need birth control anymore (due to lack of desire for sex) and such side effects can last years after discontinuation very cool definitely not fucked up